The Challenge
The NHS has invested significantly in digitisation over the past two decades. Yet front-line clinicians often report that software systems remain inadequate, frustrating, and slow [1]. Rather than a streamlined digital environment, they face duplicated input, inconsistent interfaces, and missing features. For child health, this problem is even more pronounced. Essential paediatric functionality - such as accurate growth monitoring, structured data capture for audit, and child-specific prescribing support - is often unavailable or unfit for purpose in NHS IT systems. Historically, children and young people are underrepresented in health tech innovation [2] and existing market incentives tend to compound, rather than redress, this imbalance.
This persistent gap is not simply the result of underinvestment. Rather, it reflects a structural failure in how digital health technology is developed and deployed.
Software suppliers understandably prioritise areas with greater commercial return and lower regulatory complexity. This often results in features vital to child health being delayed or entirely omitted from systems on which clinicians rely. This is compounded because the NHS must pay repeatedly to build the same features across each of the clinical systems in use. This is wasteful of taxpayer funds, and the lack of standardisation in clinical interfaces undermines clinical safety and our ability to train new clinicians.
This is an example of market failure, but the NHS is not well configured to address this failure. Despite having vast economic scale, and enjoying an unique position as the centrepiece of the UK’s social welfare apparatus [3], the NHS fails to exploit these strengths to own and drive the delivery of healthcare technology.
Another contributing factor is the frequent organisational restructuring of the NHS, both centrally and regionally. The most recent of these reforms, announced in February 2025, imposes 50% cuts on Integrated Care Boards and merges NHS England into the Department of Health and Social Care, both of which changes have resulted in significant slowing of organisational decision-making.
In this climate, long-term NHS technical infrastructure projects struggle to gain traction or retain continuity. Funding streams for projects are often threatened or even cut off abruptly, and the result over decades is a patchwork of incompatible systems, local workarounds, and one-off pilots, few of which achieve sustained impact at scale.
In other parts of the technology industry, their ‘best practices’ can be shared through modular, reusable infrastructural components. These form the ‘hidden infrastructure’ of the digital world. They enable services like encrypted web browsing, weather updates, global navigation, secure payments, and logistics to be developed quickly, consistently, and at scale.
Globally, the healthcare IT industry, and within that the NHS, has failed to build this kind of shared infrastructure, and the absence of it increases both the cost and the risk of innovation, as well as causing unacceptable variation in the quality of clinical user interfaces and generally low availability of quality digital clinical tools. Healthcare software has eschewed modern technical architecture in favour of “silos”, and “one system” approaches, which make integration and solving problems with shared infrastructure impossible.
“Communities of practice”, clinical user groups and local customisations within the “walled garden” of a single proprietary clinical system are the antithesis of progress. They represent a way for vendors to have captive clinician users refine their products, but those insights cannot usually be shared across different clinical systems, cannot be shared openly, and indeed often cannot even be shared easily between two different instances of the same clinical system at different NHS sites.
The Solution
Recognising these problems, the Royal College of Paediatrics and Child Health (RCPCH) established the RCPCH Incubator in 2020, bringing together clinicians, software developers, academics and users to develop safe, reusable, open-source digital tools for child health. As a charity, the Incubator can be guided by clinical need, safety, ethical standards, equity of access, and ubiquity.
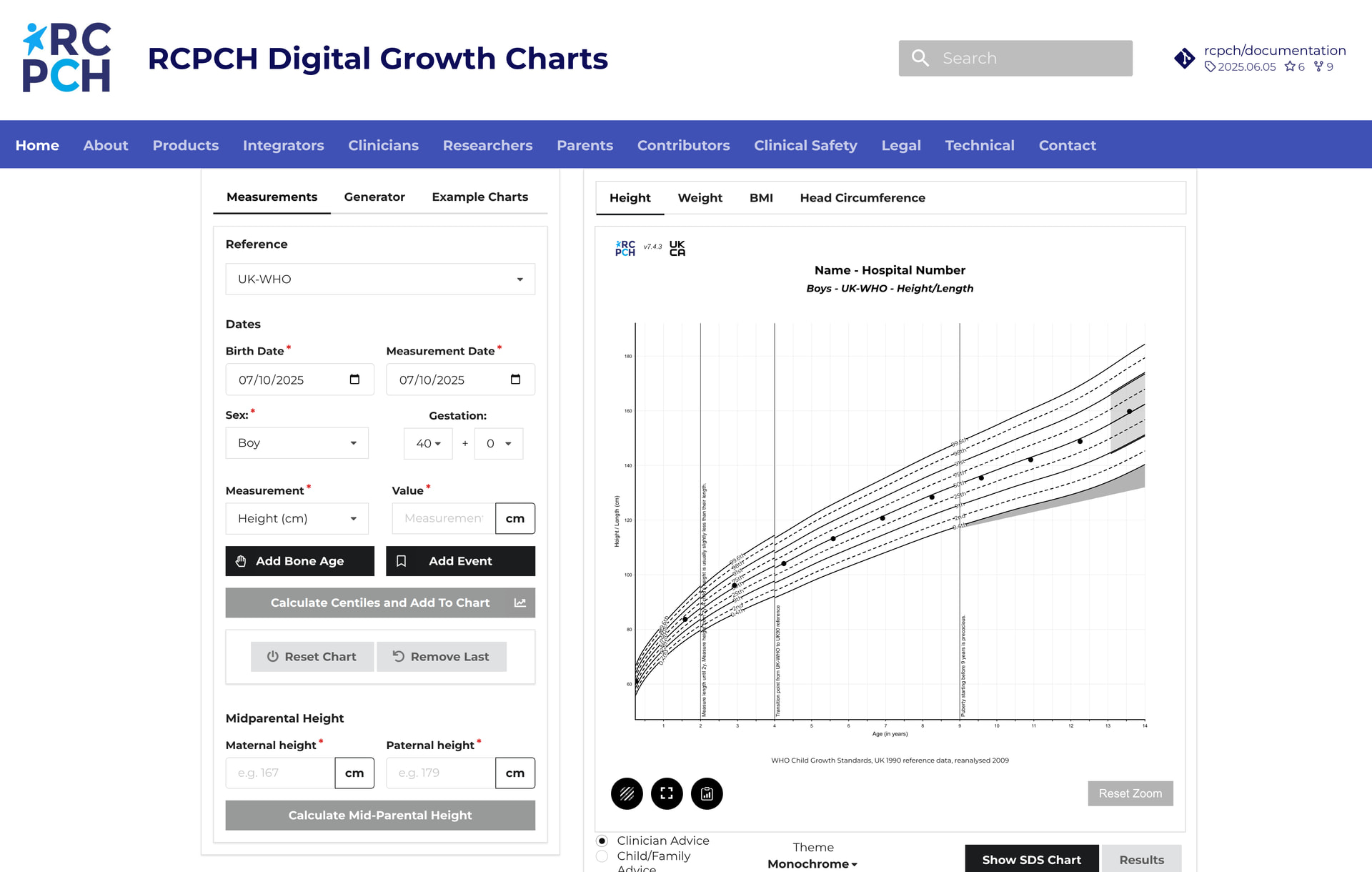
The Incubator’s first and most prominent project to date is the Digital Growth Charts platform. Paediatric growth monitoring in the UK requires complex statistical calculations based on UK90 and WHO reference datasets. Historically, the health IT market has largely failed to implement fit-for-purpose growth parameter calculation and charting software, because it is difficult to implement the required calculations.
The RCPCH Digital Growth Charts platform provides an authoritative, low-cost web service that performs growth calculations accurately and returns structured data results for use in electronic health records [4]. The RCPCH Digital Growth Charts platform is live and is already integrated into many UK primary and secondary care settings including all NHS Trusts within Wales. It is a registered medical device, has full and open documentation [5], and the charts it produces are standardised, accurate, and aligned with College-endorsed guidance.
Figure 1 RCPCH Digital Growth Charts
Beyond growth charts, the Incubator now supports a growing portfolio of projects. These include the Epilepsy12 and National Paediatric Diabetes Audit platforms, the MindTheGap Transition Community of Practice [6], and an early-stage tool for assessing social determinants of health.. Where the market has failed to deliver these tools, the Incubator builds them - safely, rapidly, and sustainably.
This new and readily transferable model of clinical software development side-steps many of the challenges described above, and presents an opportunity to update the role of professional medical bodies across the UK and internationally. We are not aware of any other medical standard-setting body working in this way anywhere in the world.
Traditionally our Royal Colleges have focused on standard-setting, education, examinations, and advocacy in the form of documents and PDFs published on websites, but in a digital age this is no longer sufficient. For the future, clinical guidance will need to be clinically authored but can be disseminated as code - machine-readable, peer-reviewed, openly implemented, and embeddable into clinical workflows to have real-world impact.
We call this paradigm “Royal Colleges 3.0” - a vision in which Colleges become stewards of Best Practice as Code.
Medical Colleges are uniquely positioned to fulfil this role. They already have longevity, clinical authority, trust, and legitimacy. They often have non-profit status and global reach. Unlike private companies, they are not excessively influenced by commercial considerations. Adding the necessary technical capacity, resourcing and governance, Colleges should become developers and custodians of digital clinical infrastructure.
This is not a call for Colleges to replace the health technology sector, but to fill gaps the market cannot. Just as the Colleges have always set written standards for clinical practice, they can now set standards through direct digital implementations - indeed this is a solid strategy for increasing Colleges’ relevance in a technological age.
At a time when proprietary clinical digital tools and closed AI models may threaten to make significant parts of the knowledge-base of medicine permanently the property of a corporation, the open-source, Collegiate model we demonstrate is a credible alternative future.
Trusted clinical institutions such as Royal Colleges can take an active role in shaping the digital tools of the future - not only for paediatrics, but potentially across all specialties. We believe that this model can and should be replicated by other Royal Colleges and similar standard-setting bodies, nationally and internationally.
ACKNOWLEDGMENTS
No prior publications of this article
COMPETING INTERESTS
Marcus Baw and Simon Chapman are paid software development consultants to the RCPCH.
REFERENCES
[1] Atul Gawande. Why Doctors Hate Their Computers. The New Yorker, Nov 5, 2018. Available from: https://www.newyorker.com/magazine/2018/11/12/why-doctors-hate-their-computers
[2] NHS England - Structure of the NHS, Version 1, 9 November 2022 https://www.england.nhs.uk/long-read/structure-of-the-nhs/ (accessed 30th May 2025)
[3] Wright CM, Chapman S, Cole TJ. How can we best chart children’s growth in the paperless age? The UK experience. Arch Dis Child. 2024 Jan 22;109(2):78-82. http://dx.doi.org/10.1136/archdischild-2023-325363. PMID: 37463736
[4] RCPCH Digital Growth Charts API demonstration and documentation website. https://growth.rcpch.ac.uk
[5] NIHR MindTheGap Transition Platform. https://mindthegap-transition.org